Minnesota Severe Mental Illness Information, Laws, & Helpful Resources
The term severe mental illness (SMI) includes schizophrenia spectrum disorders, severe bipolar disorder, and major depression with psychotic features. These disorders put an individual at high risk for criminalization and preventable tragedies such as victimization and suicide. Every state has different laws and policies around accessing treatment for SMI and some states have more resources and treatment options than others. Here you will find state-specific resources for navigating the SMI treatment system, an evaluation of local laws, as well as state SMI data and research.
Family Resources in Resources in Minnesota
- Minnesota Department of Human Services (mn.gov) Resources and contacts
- Understanding the Minnesota Civil Commitment Process (namimn.org) Overview of the eight steps in the commitment process
- NAMI Minnesota (namimn.org) Support groups, training, information
- Minnesota Disability Law Center (mylegalaid.org) Free civil legal assistance to individuals with disabilities
- Homeless Information: Minnesota | U.S. Department of Housing and Urban Development (hud.gov/states/minnesota) Find help hotlines, financial assistance, foodbanks, and shelters by city or county
- Minnesota Offender Search (coms.doc.state.mn.us) Find a prison inmate by name or MNDOC number
- Minnesota State Bar Association (mnbar.org) Legal Assistance
How many people in Minnesota have SMI?
individuals with severe mental illness.
individuals with SMI who receive treatment in a given year.
of the adult population is estimated living with a SMI in the United States.
State psychiatric hospital beds in Minnesota
2023 total beds: 192
- Civil beds: 192
- All patients committed to state hospitals in Minnesota are committed as civil patients, including those who have been charged with crimes.
2023 beds per 100,000 people: 3.4
Click here for more information about state psychiatric hospital beds in Minnesota.
A minimum of 50 beds per 100,000 people is considered necessary to provide minimally adequate treatment for individuals with severe mental illness. Minnesota fails to meet this minimum standard.
For Additional Information
Data is a powerful tool to advocate for change. Curious about a specific data point in your state? Reach out to us at ORPA@treatmentadvocacycenter.org
Fast Facts on SMI in Minnesota
Deinstitutionalization, outdated treatment laws, discriminatory Medicaid funding practices, and the prolonged failure by states to fund their mental health systems drive those in need of care into the criminal justice and corrections systems.
20%
2,959
192
15 to 1
2021 Minnesota State Mental Health Agency's expenditures
Every state receives block grant funding from the federal government to provide mental health services to their community. Below is some information about how these dollars are spent and compares to other state spending.
2021 data not available
2021 data not available
2021 data not available
2021 data not available
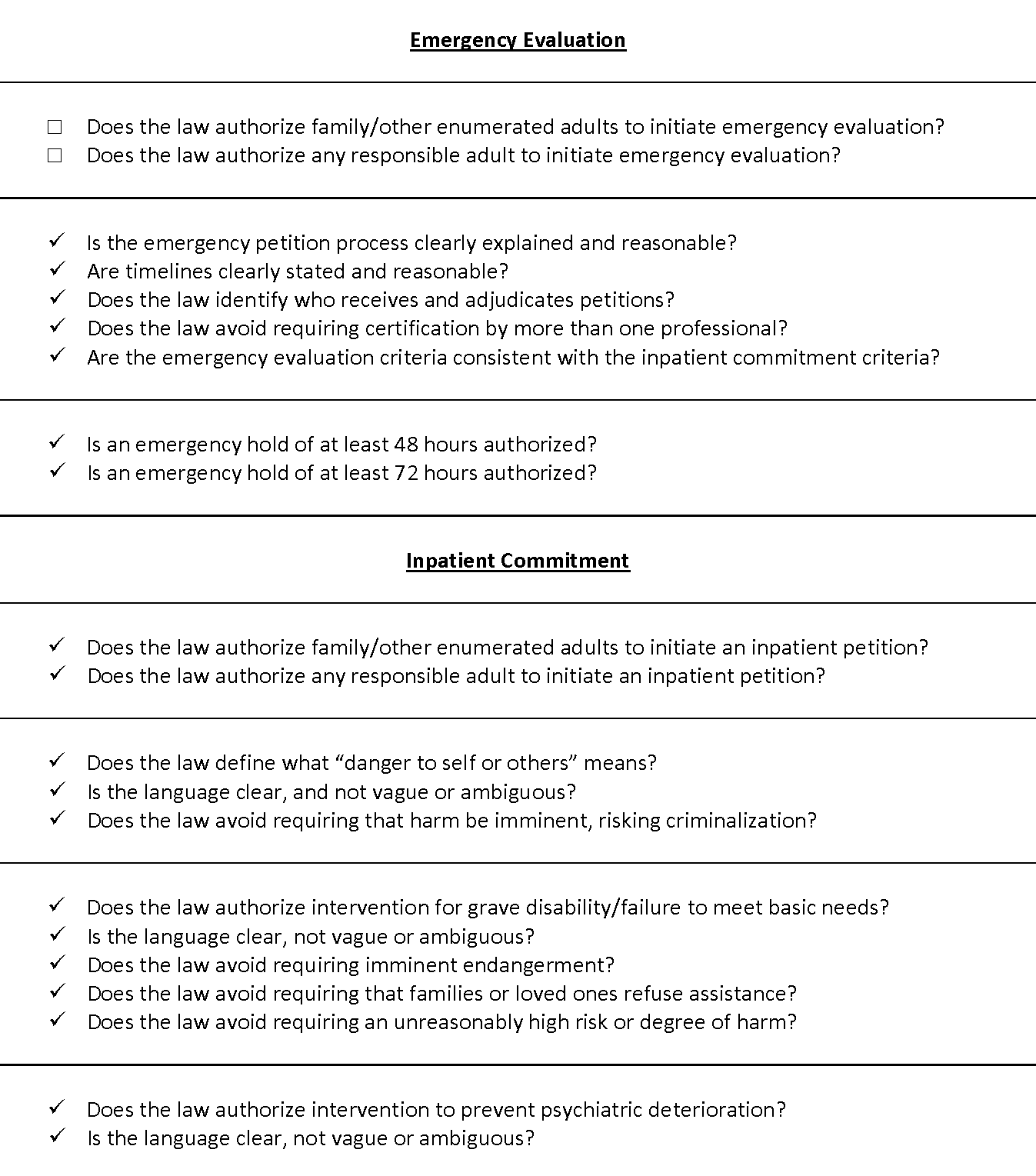
Minnesota's Treatment Laws
MINN. STAT. § 253B.051(1)(a). If a peace officer or health officer has reason to believe, either through direct observation of the person’s behavior or upon reliable information of the person’s recent behavior and, if available, knowledge or reliable information concerning the person’s past behavior or treatment that the person: 1. has a mental illness or developmental disability and is in danger of harming self or others if the officer does not immediately detain the patient, the peace officer or health officer may take the person into custody and transport the person to an examiner or a treatment facility, state-operated treatment program, or community-based treatment program;
MINN. STAT. § 253B.07(2)(a). Any interested person, except a member of the prepetition screening team, may file a petition for commitment in the district court of the county of financial responsibility or the county where the proposed patient is present. If the head of the treatment facility, state-operated treatment program, or community-based treatment program believes that commitment is required and no petition has been filed, that person shall petition for the commitment of the proposed patient. MINN. STAT. § 253B.09. Subdivision 1. Standard of proof.— (a) If the court finds by clear and convincing evidence that the proposed patient is a person who poses a risk of harm due to mental illness, or is a person who has a developmental disability or chemical dependency, and after careful consideration of reasonable alternative dispositions including but not limited to dismissal of petition; voluntary outpatient care; voluntary admission to a treatment facility, state-operated treatment program, or community-based treatment program; appointment of a guardian or conservator; or release before commitment as provided for in subdivision 4, it finds that there is no suitable alternative to judicial commitment, the court shall commit the patient to the least restrictive treatment program or alternative programs which can meet the patient’s treatment needs consistent with section 253B.03, subdivision 7. (b) In deciding on the least restrictive program, the court shall consider a range of treatment alternatives including but not limited to community-based nonresidential treatment, community residential treatment, partial hospitalization, acute care hospital, assertive community treatment teams, and state-operated treatment programs. The court shall also consider the proposed patient’s treatment preferences and willingness to participate voluntarily in the treatment ordered. The court may not commit a patient to a facility or program that is not capable of meeting the patient’s needs. (c) If, after careful consideration of reasonable alternative dispositions, the court finds no suitable alternative to judicial commitment and the court finds that the least restrictive alternative as determined in paragraph (a) is a treatment facility or community-based treatment program that is less restrictive or more community based than a state-operated treatment program, and there is a treatment facility or a community-based treatment program willing to accept the civilly committed patient, the court may commit the patient to both the treatment facility or community-based treatment program and to the commissioner, in the event that treatment in a state-operated treatment program becomes the least restrictive alternative. If there is a change in the patient’s level of care, then: 1) if the patient needs a higher level of care requiring admission to a state-operated treatment program, custody of the patient and authority and responsibility for the commitment may be transferred to the commissioner for as long as the patient needs a higher level of care; and 2) when the patient no longer needs treatment in a state-operated treatment program, the program may provisionally discharge the patient to an appropriate placement or release the patient to the treatment facility or community-based treatment program if the program continues to be willing and able to readmit the patient, in which case the commitment, its authority, and responsibilities revert to the non-state-operated treatment program. Both agencies accepting commitment shall coordinate admission and discharge planning to facilitate timely access to the other’s services to meet the patient’s needs and shall coordinate treatment planning consistent with section 253B.03, subdivision 7. (d) If a person is committed to a state-operated treatment program as a person who poses a risk of harm due to mental illness or as a person who has a developmental disability or chemical dependency, the court shall order the commitment to the commissioner. The commissioner shall designate the placement of the person to the court. (e) If the court finds a proposed patient to be a person who poses a risk of harm due to mental illness under section 253B.02, subdivision 13, clause (4), the court shall commit the patient to a treatment facility or community-based treatment program that meets the proposed patient’s needs. MINN. STAT. § 253B.02. Subd. 13. Person who poses a risk of harm due to a mental illness. (a) A “person who poses a risk of harm due to a mental illness” means any person who has an organic disorder of the brain or a substantial psychiatric disorder of thought, mood, perception, orientation, or memory that grossly impairs judgment, behavior, capacity to recognize reality, or to reason or understand, that is manifested by instances of grossly disturbed behavior or faulty perceptions and who, due to this impairment, poses a substantial likelihood of physical harm to self or others as demonstrated by: (1) a failure to obtain necessary food, clothing, shelter, or medical care as a result of the impairment; (2) an inability for reasons other than indigence to obtain necessary food, clothing, shelter, or medical care as a result of the impairment and it is more probable than not that the person will suffer substantial harm, significant psychiatric deterioration or debilitation, or serious illness, unless appropriate treatment and services are provided; (3) a recent attempt or threat to physically harm self or others; or (4) recent and volitional conduct involving significant damage to substantial property. (b) A person does not pose a risk of harm due to mental illness under this section if the impairment is solely due to: (1) epilepsy; (2) developmental disability; (3) brief periods of intoxication caused by alcohol, drugs, or other mind-altering substances; or (4) dependence upon or addiction to any alcohol, drugs, or other mind-altering substances. MINN. STAT. § 253B.18(1) (a) Upon the filing of a petition alleging that a proposed patient is a person who has a mental illness and is dangerous to the public, the court shall hear the petition as provided in sections 253B.07 and 253B.08. If the court finds by clear and convincing evidence that the proposed patient is a person who has a mental illness and is dangerous to the public, it shall commit the person to a secure treatment facility or to a treatment facility or state-operated treatment program willing to accept the patient under commitment. The court shall commit the patient to a secure treatment facility unless the patient or others establish by clear and convincing evidence that a less restrictive state-operated treatment program or treatment facility is available that is consistent with the patient’s treatment needs and the requirements of public safety. In any case where the petition was filed immediately following the acquittal of the proposed patient for a crime against the person pursuant to a verdict of not guilty by reason of mental illness, the verdict constitutes evidence that the proposed patient is a person who has a mental illness and is dangerous to the public within the meaning of this section. The proposed patient has the burden of going forward in the presentation of evidence. The standard of proof remains as required by this chapter. Upon commitment, admission procedures shall be carried out pursuant to section 253B.10. (b) Once a patient is admitted to a treatment facility or state-operated treatment program pursuant to a commitment under this subdivision, treatment must begin regardless of whether a review hearing will be held under subdivision 2. MINN. STAT. § 253B.02(17). Person who has a mental illness and is dangerous to the public. — A “person who has a mental illness and is dangerous to the public” is a person: (1) who has an organic disorder of the brain or a substantial psychiatric disorder of thought, mood, perception, orientation, or memory that grossly impairs judgment, behavior, capacity to recognize reality, or to reason or understand, and is manifested by instances of grossly disturbed behavior or faulty perceptions; and (2) who as a result of that impairment presents a clear danger to the safety of others as demonstrated by the facts that (i) the person has engaged in an overt act causing or attempting to cause serious physical harm to another and (ii) there is a substantial likelihood that the person will engage in acts capable of inflicting serious physical harm on another.
Recommended updates to treatment laws
- 1
Amend Minn. Stat. § 253B.051(1)(a) to authorize citizen right of petition for at least enumerated citizens, preferably any responsible adult, for emergency evaluation
- 2
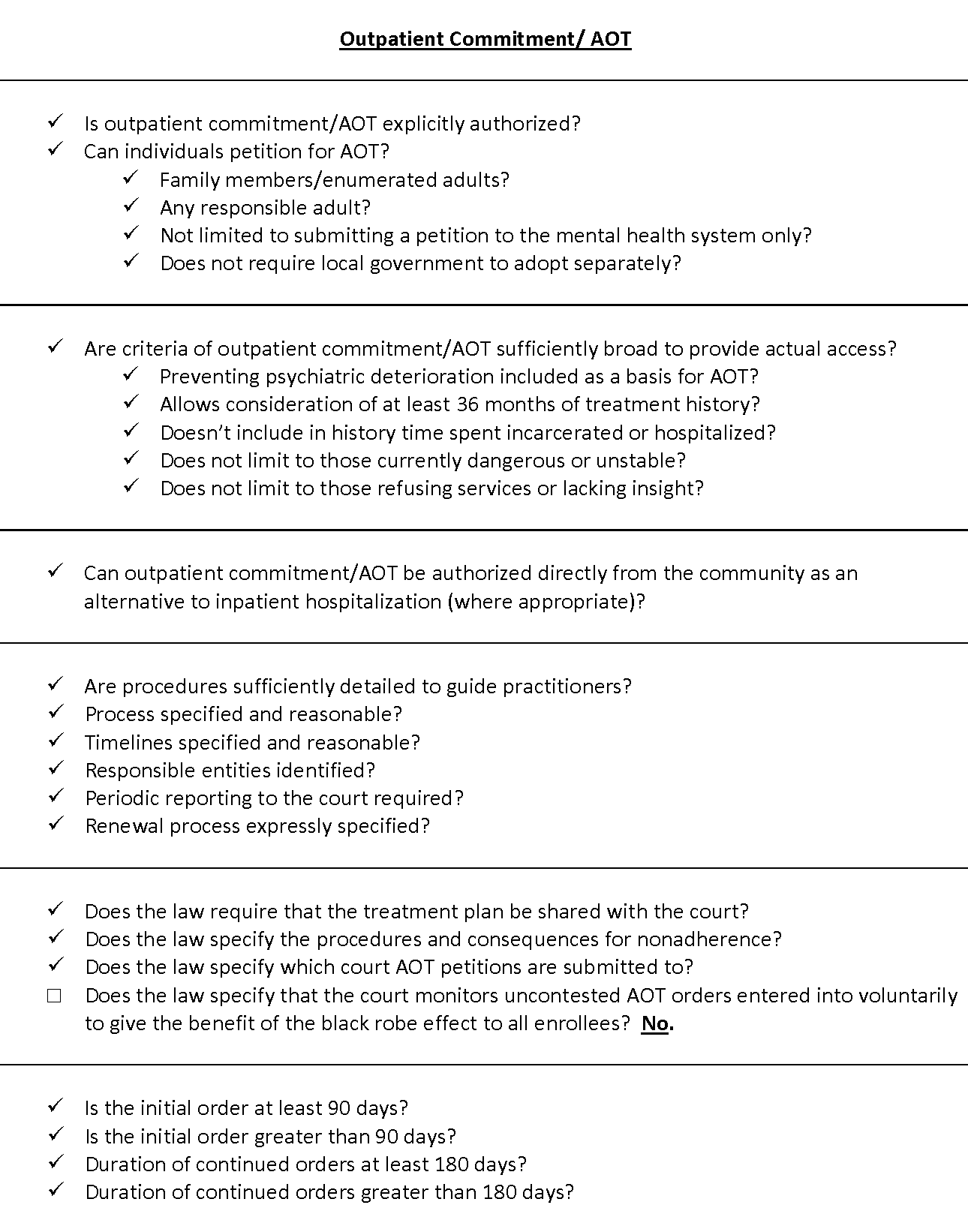
Adopt express procedures for the court to monitor uncontested AOT orders entered into voluntarily to give the benefit of the black robe effect to all enrollees